Eric S. Langer, BioPlan Associates03.07.17
Hiring has become increasingly challenging as new technologies and integration of better bioprocess put greater demands on staff training and hiring. Biomanufacturing improvements demand different skill sets as well as understanding how novel technologies at R&D scale may not be feasible at commercial scale. One such area is in cell therapy manufacturing, where current bioprocessing strategies are going to be bottlenecked by the lack of trained staff.
Other areas, such as continuous processing devices, expanding automation, multi-column, computer-controlled downstream purification, and implementing flexible bioprocessing facilities will be throttled by the inability to hire and train operators to run these new processes. Staff training to ensure productivity will lag and be outstripped by the lack of available expertise. Some of the first to be hit by hiring constraints will be the contract manufacturing organizations (CMOs) where multiple products and campaigns are run, and new technologies are often first introduced.
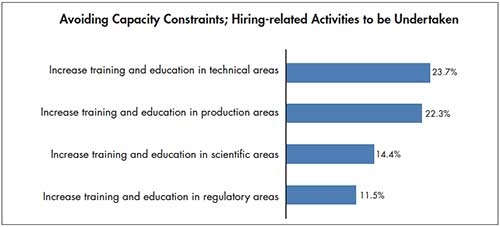
As the demand for innovation in biomanufacturing continues, the investment considerations must also be made for ensuring staff expertise and training. According to BioPlan Associates’, “13th Annual Report and Survey of Biopharmaceutical Manufacturing Capacity and Production,”1 of the 222 qualified industry executives, we found that about 1 in 4 bioprocessing professionals see what is coming down the pike, and recognize the need to address their training and hiring to avoid capacity constraints (see Figure 1).
Industry segments likely to be hit hardest
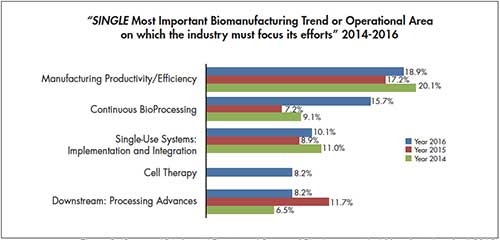
One of the bioprocessing segments likely to be hit the hardest is in cell therapy. This innovative field is emerging as one of the most important trends (see Figure 2). In 2016, the segment was noted as the fourth most important biomanufacturing trend area. This is significant, considering the small size of these industry sectors. Further, very few mainstream biopharmaceutical professionals have had any actual involvement with these products, so it is not unexpected that this was the first year that cell therapy made the list.
Better manufacturing technologies needed
A number of innovative cellular and gene therapies are in development, and R&D and investments in these fields are rapidly growing. Although approvals and markets remain very small, by the standards of the mainstream (bio)pharmaceutical industry, this is likely to change as the first clinical trials are successfully concluded. And although today, the vast majority of cell and gene therapies in development are targeted to orphan, often super-orphan, indications, this is going to change as well.
Many developers today are academic spin-off research facilities, and some are primarily interested in showing proof-of-principle. Thus, there is a lack of needed expertise in development of manufacturing platforms appropriate for broad, large-market cell therapies. Manufacturing technologies currently used for most cell and gene therapies are often open (vs. closed, aseptic) systems, e.g., manual pipetting with cell cultured in flasks, roller bottles, etc., rather than modern bioreactors. Cell isolation, manipulation and culture remains yet to be automated, and current manufacturing is labor-intensive and expensive.
For example, a single autologous—using patient’s own cells for return to that patient—unit often requires weeks of work by multiple staff in a dedicated cleanroom. This is among the reasons that make cell and gene therapies very expensive. Compared to current therapeutics, many or most cell and gene therapies will be curative with a single dose or single manufactured unit. This need for only a single one-time dose combined with unprecedented high costs for manufacturing, could lead insurers to avoid reimbursing for these therapies for which COGs of a single unit alone are roughly comparable with those for a commercial-scale bioreactor run producing many thousands of doses.
There is also a general lack of industry knowledge about how companies will actually commercially manufacture cell therapy products in development. Further, making these cost-effective will be critical for both patients and payers. With current total cell/gene therapy production around 10,000 patient units/year, orders of magnitude growth in manufacturing capacity will be needed, first for later-stage trials and then even more for commercial manufacturing.
Staffing problems ahead
Staffing problems are likely to outstrip issues like facility or cleanroom availability. Manufacturing expertise, or lack thereof, is likely a future bottleneck for growth in cell and gene therapies. Manufacturing live cells as end products is much more complex than producing non-living proteins, antibodies, etc. Bioprocessing professionals with experience in cell and gene therapies are relatively rare today. And gene/cell therapy manufacturing-related positions need high levels of expertise, despite often being repetitive and stressful. Today, staff appear to be over-qualified and it has been reported that six months of additional training is needed, even for currently trained bioprocessing staff. Process development staff for cell and gene therapies are particularly in short supply (see Figure 3).
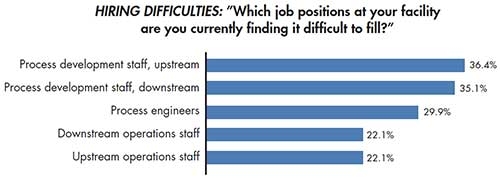
In our study, we asked respondents to identify job positions at their facility they are currently having difficulty filling. Process development (PD) jobs topped the list, led by upstream PD staff (36.4%) and downstream PD staff (35.1%). Also within the top five jobs most challenging to hire for were process engineers (29.9%), downstream operations staff (22.1%) and upstream operations staff (22.1%).
In cell and gene therapy, this on-going hiring challenge will further confound growth of manufacturing capacity to levels needed to support even just a few non-orphan-type products. And many industry observers have described a pending capacity crunch, if and when product approvals occur. CMOs and others involved in cell and gene therapies are likely to experience increased demand, so manufacturing capacity may be at a premium in coming years, as available staff keep busy.
We can also expect a large number of new players to enter the field in coming years, particularly if new technologies and automation provide viable options for cost-effective commercial manufacturing. Yet even here, staffing to ensure technical expertise is on-hand will be a challenge.
The manufacturing capacity situation with cell and gene therapies could be likened to the monoclonal antibodies industry sector in the early 1990s, when the industry faced potentially very serious capacity crunches. Even all available/idle worldwide capacity at the time was not sufficient to manufacture what would be needed to support just a few blockbuster (>$1 billion/year) products. At the time, developers and CMOs responded by constructing many ≥100,000 L manufacturing facilities anchored by multiple ≥10,000 L bioreactors. Growth in cell and gene therapies manufacturing, if supported by comparable expansion of bioprocessing infrastructure, could be even quicker than the monoclonal antibodies capacity expansion.
Ultimately, the industry will respond by building needed facilities, automation and capacity. However, the availability of trained staff to run these high-tech operations may be the slowest bottleneck to resolve. In particular, the many small companies dominating the cell therapy field will have few viable options for cost-effectively manufacturing their products for large, commercially viable markets. Cell and gene therapies have a very promising future, and these therapies could revolutionize many disease treatments. But a lot of work remains to prepare for this, and hiring difficulties aren’t going away. CP
References
Eric S. Langer
BioPlan Associates
Eric S. Langer is president and managing partner at BioPlan Associates, Inc., a biotechnology and life sciences marketing research and publishing firm established in Rockville, MD in 1989. He is editor of numerous studies, including “Biopharmaceutical Technology in China,” “Advances in Large-scale Biopharmaceutical Manufacturing”, and many other industry reports. elanger@bioplanassociates.com 301-921-5979. www.bioplanassociates.com
Other areas, such as continuous processing devices, expanding automation, multi-column, computer-controlled downstream purification, and implementing flexible bioprocessing facilities will be throttled by the inability to hire and train operators to run these new processes. Staff training to ensure productivity will lag and be outstripped by the lack of available expertise. Some of the first to be hit by hiring constraints will be the contract manufacturing organizations (CMOs) where multiple products and campaigns are run, and new technologies are often first introduced.
As the demand for innovation in biomanufacturing continues, the investment considerations must also be made for ensuring staff expertise and training. According to BioPlan Associates’, “13th Annual Report and Survey of Biopharmaceutical Manufacturing Capacity and Production,”1 of the 222 qualified industry executives, we found that about 1 in 4 bioprocessing professionals see what is coming down the pike, and recognize the need to address their training and hiring to avoid capacity constraints (see Figure 1).
Industry segments likely to be hit hardest
One of the bioprocessing segments likely to be hit the hardest is in cell therapy. This innovative field is emerging as one of the most important trends (see Figure 2). In 2016, the segment was noted as the fourth most important biomanufacturing trend area. This is significant, considering the small size of these industry sectors. Further, very few mainstream biopharmaceutical professionals have had any actual involvement with these products, so it is not unexpected that this was the first year that cell therapy made the list.
Better manufacturing technologies needed
A number of innovative cellular and gene therapies are in development, and R&D and investments in these fields are rapidly growing. Although approvals and markets remain very small, by the standards of the mainstream (bio)pharmaceutical industry, this is likely to change as the first clinical trials are successfully concluded. And although today, the vast majority of cell and gene therapies in development are targeted to orphan, often super-orphan, indications, this is going to change as well.
Many developers today are academic spin-off research facilities, and some are primarily interested in showing proof-of-principle. Thus, there is a lack of needed expertise in development of manufacturing platforms appropriate for broad, large-market cell therapies. Manufacturing technologies currently used for most cell and gene therapies are often open (vs. closed, aseptic) systems, e.g., manual pipetting with cell cultured in flasks, roller bottles, etc., rather than modern bioreactors. Cell isolation, manipulation and culture remains yet to be automated, and current manufacturing is labor-intensive and expensive.
For example, a single autologous—using patient’s own cells for return to that patient—unit often requires weeks of work by multiple staff in a dedicated cleanroom. This is among the reasons that make cell and gene therapies very expensive. Compared to current therapeutics, many or most cell and gene therapies will be curative with a single dose or single manufactured unit. This need for only a single one-time dose combined with unprecedented high costs for manufacturing, could lead insurers to avoid reimbursing for these therapies for which COGs of a single unit alone are roughly comparable with those for a commercial-scale bioreactor run producing many thousands of doses.
There is also a general lack of industry knowledge about how companies will actually commercially manufacture cell therapy products in development. Further, making these cost-effective will be critical for both patients and payers. With current total cell/gene therapy production around 10,000 patient units/year, orders of magnitude growth in manufacturing capacity will be needed, first for later-stage trials and then even more for commercial manufacturing.
Staffing problems ahead
Staffing problems are likely to outstrip issues like facility or cleanroom availability. Manufacturing expertise, or lack thereof, is likely a future bottleneck for growth in cell and gene therapies. Manufacturing live cells as end products is much more complex than producing non-living proteins, antibodies, etc. Bioprocessing professionals with experience in cell and gene therapies are relatively rare today. And gene/cell therapy manufacturing-related positions need high levels of expertise, despite often being repetitive and stressful. Today, staff appear to be over-qualified and it has been reported that six months of additional training is needed, even for currently trained bioprocessing staff. Process development staff for cell and gene therapies are particularly in short supply (see Figure 3).
In our study, we asked respondents to identify job positions at their facility they are currently having difficulty filling. Process development (PD) jobs topped the list, led by upstream PD staff (36.4%) and downstream PD staff (35.1%). Also within the top five jobs most challenging to hire for were process engineers (29.9%), downstream operations staff (22.1%) and upstream operations staff (22.1%).
In cell and gene therapy, this on-going hiring challenge will further confound growth of manufacturing capacity to levels needed to support even just a few non-orphan-type products. And many industry observers have described a pending capacity crunch, if and when product approvals occur. CMOs and others involved in cell and gene therapies are likely to experience increased demand, so manufacturing capacity may be at a premium in coming years, as available staff keep busy.
We can also expect a large number of new players to enter the field in coming years, particularly if new technologies and automation provide viable options for cost-effective commercial manufacturing. Yet even here, staffing to ensure technical expertise is on-hand will be a challenge.
The manufacturing capacity situation with cell and gene therapies could be likened to the monoclonal antibodies industry sector in the early 1990s, when the industry faced potentially very serious capacity crunches. Even all available/idle worldwide capacity at the time was not sufficient to manufacture what would be needed to support just a few blockbuster (>$1 billion/year) products. At the time, developers and CMOs responded by constructing many ≥100,000 L manufacturing facilities anchored by multiple ≥10,000 L bioreactors. Growth in cell and gene therapies manufacturing, if supported by comparable expansion of bioprocessing infrastructure, could be even quicker than the monoclonal antibodies capacity expansion.
Ultimately, the industry will respond by building needed facilities, automation and capacity. However, the availability of trained staff to run these high-tech operations may be the slowest bottleneck to resolve. In particular, the many small companies dominating the cell therapy field will have few viable options for cost-effectively manufacturing their products for large, commercially viable markets. Cell and gene therapies have a very promising future, and these therapies could revolutionize many disease treatments. But a lot of work remains to prepare for this, and hiring difficulties aren’t going away. CP
|
Cellular therapies involve the culture of cells, usually from humans, for therapeutic administration. Gene therapies involve the use of genetic vectors to genetically transform cells for therapeutic administration, either ex vivo gene therapy, where cells are transformed, cultured and cells administered to patients, the current predominant approach, and in vivo gene therapy, where the genetic vectors are administered directly into patients. Further, cell/gene therapies may be classed based on their source/methods of manufacturing, with autologous cell/gene therapies involving administration of the patient’s own cultured cells and allogeneic cell/gene therapies involving administration of the same cells to multiple patients, with their manufacture involving batches/lots larger than 1 patient unit. |
References
- 13th Annual Report and Survey of Biopharmaceutical Manufacturing Capacity and Production, BioPlan Associates, Inc. Rockville, MD., April 2016.
Eric S. Langer
BioPlan Associates
Eric S. Langer is president and managing partner at BioPlan Associates, Inc., a biotechnology and life sciences marketing research and publishing firm established in Rockville, MD in 1989. He is editor of numerous studies, including “Biopharmaceutical Technology in China,” “Advances in Large-scale Biopharmaceutical Manufacturing”, and many other industry reports. elanger@bioplanassociates.com 301-921-5979. www.bioplanassociates.com















