
Ben Locwin, Healthcare Science Advisors07.18.17
It’s been a busy few months in the pharma world, after a tremendously successful inaugural launch of CPhI North America in May, DIA’s annual conference, BIO2017, and others. Interestingly, I just returned from chairing another healthcare conference where the topic I fielded most often once again wasn’t been about safety or efficacy of different treatments, or new treatments for underserved conditions, it’s drug pricing. The public outcry over drug prices and pricing trends ebbs and flows a bit with the latest news story on the topic, but the sensitivity to the situation is at an all-time high. Our industry is in a risky position at the moment, and it’s going to take all of us working together to improve our future.
Innovation and cross-cutting themes are nice, but what am I going to be paying?
A lot of conferences in healthcare continue to bring in subject matter experts on topics such as innovative approaches to clinical development, new quality metrics and parameters, improved assay sensitivity, designing better clinical trials, and novel approaches to gene therapies for personalized medicine. Great topics all, but at this moment, the social pressure (via groupthink in social media platforms) is squarely on affordability of healthcare and the prices set for drug therapies. Other work within pharma innovation may indeed be helping the industry progress against current expectations of Wall Street, but very soon that balance will shift and pharma’s continued market success will hinge upon how transparency of pricing and affordability translate tangibly to consumers on Main Street. Remember, pricing has ramifications that ripple everywhere: From pricing pressures on CROs, CDMOs, CMOs, and suppliers working with brand drug companies, changes to the assignment of drug tiers within prescription healthcare insurance plans, prices hospitals pay for drugs and then charge-forward to the patient, etc.
We should all be quite concerned, because working within the industry, to the outsiders, we are all considered part of Big Pharma. The issue right now is one of reputation management, perceived morality and ethics, and improving our customers’ perceptions of us.
Here’s something that should be a top concern about contemporary drug pricing: That no matter what the price is set at for a particular drug product, even if it’s subjectively “a good value,” the public has been conditioned by the media to have a tremendous level of mistrust—perhaps rightly so in some cases—and they’ll think that they’re still being played by Big Pharma. So there needs to be a branding overhaul of what the industry is, or should be, about. The consumers and patients—let’s not mince words, we’re all consumers of healthcare—won’t notice marginal price decrements on their prescriptions even if companies do this voluntarily on a broad basis. There needs to be an appeal to the public that the industry is taking patients’ concerns seriously, and right now one of their top concerns is pricing.
With liberty and surge pricing for all
One of the concepts that I’ve brought to pharma companies’ strategic pricing practices is that of surge pricing, also called dynamic pricing models, like the kind used by ride sharing services Uber and Lyft—called Prime Time pricing—and others.
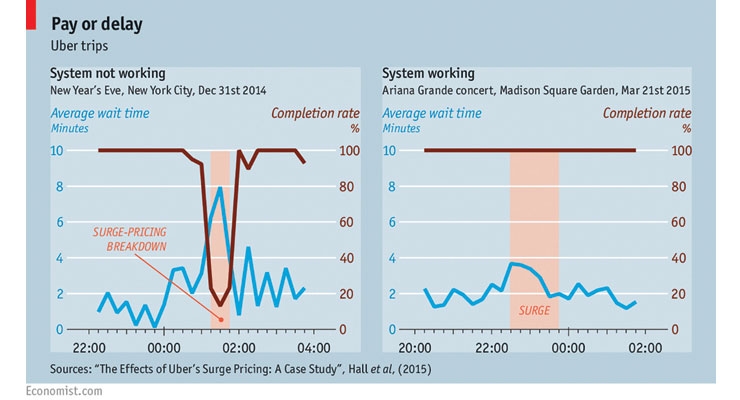
How does it work? Surge pricing looks at the elasticity of demand, and when demand rises, pricing increases as well to re-normalize at a point where the free market determines the ‘value’ of the product or service exists. The Economist published the following Figure1 on the previous page, showing how surge pricing works. On the left side, the market was failed when Uber’s surge pricing algorithm became unresponsive (defective) for a short period of time in New York City on New Year’s Eve 2014. Then the right side of the figure shows how the system worked during and after an Ariana Grande concert in NYC 2015.
So on the right side of the figure, the dynamic pricing model shows that as demand fluctuates and increases, so too does the price rider-seekers will pay for their ride. Uber’s surge pricing was in-effect during the pink shaded vertical area. Sometimes this can be a 300% increase in price for a ride or more. This tends to lead to an increase in the availability of drivers based on incentivization. Quite simply, it encourages more drivers to get on the road, which in turn reduces the average person’s wait time back to nominal levels. To be sure, surge pricing approaches have been both lauded and reviled.
What is clear in this industry is that all pharmaceutical companies are for-profit entities, and therefore are invested in maximizing profit for their shareholders. Pharma as an industry has a significant R&D process and spend to fill pipelines with next-generation therapies, and many of these candidates will fail long before ever reaching the market. This financing of probabilities is extraordinarily expensive, and companies need to recoup their losses by establishing rational prices for the drugs that actually do succeed in gaining regulatory approval.
Dynamic pricing is one method of ensuring that companies stay competitive with the market and also can fund continuous innovation. The problem that develops, of course, is that manufacturers can rig the system to ‘short’ the supply to artificially increase demand rates to set dynamic surge pricing higher. There are various ways to address this eventuality in people gaming the system, but as Fermat opined, these solutions “won’t fit in these margins.” Suffice it to say that pricing approaches can’t remain the same as they are today, or the government and regulatory bodies will indeed step in and force the hand of a less-than-desirable future state.
But of course, another question that remains is how do we set the algorithm(s) for the dynamic pricing models? A good question. There are many ways to do so, some are best practices, and some are worst practices. Before a wholesale decree that dynamic pricing can’t work for healthcare treatments, such as drug therapies, because healthcare is ‘too altruistic’ of a product or service to conform to sterile economically-driven models of supply and demand, note that Uber itself shows how raising prices to incentivize drivers can lead to more reliable ride availability when, for example, people are leaving bars and restaurants late at night and are too drunk to drive. In certain cases, the ability for drivers to be paid more during off-hours means that more drivers will provide their services to the surge demand, and there will be fewer drunk drivers on the road, reducing accidents, injuries, and fatalities.4
Of course, there are many other ways to approach this issue for the industry, but it is an issue that we in fact need to collectively address before it becomes a “change that’s done to us.” There’s a wildly different perception in the world about the nature of a medicine that has been produced by a public company, and, for example, a smartphone. Both had R&D processes, incurred rigorous testing, marketing, and scrutiny of sales performance. But while society’s social contract allows the smart device to have an arbitrarily-assigned MSRP, medicine is thought of as different. Whether right or wrong, this is the challenge we’re faced with in the court of public opinion.
References
Ben Locwin
Ben Locwin, PhD, MBA, is President of Healthcare Science Advisors. He is an expert media contact for the American Association of Pharmaceutical Scientists (AAPS) and is also on the Advisory Board for the Association for Talent Development’s (ATD) Healthcare Community of Practice, working on initiatives that are improving healthcare outcomes worldwide. Dr. Locwin has worked with several of the Top 10 pharma companies (both annual sales and market cap), and is currently creating improvements in the healthcare industry on patient-centricity. This is all critically important to the future of the industry, because we’re all (or will be) patients within the system. Improving the experience and ultimately, the outcomes, helps all of us. @BenLocwin.
Innovation and cross-cutting themes are nice, but what am I going to be paying?
A lot of conferences in healthcare continue to bring in subject matter experts on topics such as innovative approaches to clinical development, new quality metrics and parameters, improved assay sensitivity, designing better clinical trials, and novel approaches to gene therapies for personalized medicine. Great topics all, but at this moment, the social pressure (via groupthink in social media platforms) is squarely on affordability of healthcare and the prices set for drug therapies. Other work within pharma innovation may indeed be helping the industry progress against current expectations of Wall Street, but very soon that balance will shift and pharma’s continued market success will hinge upon how transparency of pricing and affordability translate tangibly to consumers on Main Street. Remember, pricing has ramifications that ripple everywhere: From pricing pressures on CROs, CDMOs, CMOs, and suppliers working with brand drug companies, changes to the assignment of drug tiers within prescription healthcare insurance plans, prices hospitals pay for drugs and then charge-forward to the patient, etc.
We should all be quite concerned, because working within the industry, to the outsiders, we are all considered part of Big Pharma. The issue right now is one of reputation management, perceived morality and ethics, and improving our customers’ perceptions of us.
Here’s something that should be a top concern about contemporary drug pricing: That no matter what the price is set at for a particular drug product, even if it’s subjectively “a good value,” the public has been conditioned by the media to have a tremendous level of mistrust—perhaps rightly so in some cases—and they’ll think that they’re still being played by Big Pharma. So there needs to be a branding overhaul of what the industry is, or should be, about. The consumers and patients—let’s not mince words, we’re all consumers of healthcare—won’t notice marginal price decrements on their prescriptions even if companies do this voluntarily on a broad basis. There needs to be an appeal to the public that the industry is taking patients’ concerns seriously, and right now one of their top concerns is pricing.
With liberty and surge pricing for all
One of the concepts that I’ve brought to pharma companies’ strategic pricing practices is that of surge pricing, also called dynamic pricing models, like the kind used by ride sharing services Uber and Lyft—called Prime Time pricing—and others.
How does it work? Surge pricing looks at the elasticity of demand, and when demand rises, pricing increases as well to re-normalize at a point where the free market determines the ‘value’ of the product or service exists. The Economist published the following Figure1 on the previous page, showing how surge pricing works. On the left side, the market was failed when Uber’s surge pricing algorithm became unresponsive (defective) for a short period of time in New York City on New Year’s Eve 2014. Then the right side of the figure shows how the system worked during and after an Ariana Grande concert in NYC 2015.
So on the right side of the figure, the dynamic pricing model shows that as demand fluctuates and increases, so too does the price rider-seekers will pay for their ride. Uber’s surge pricing was in-effect during the pink shaded vertical area. Sometimes this can be a 300% increase in price for a ride or more. This tends to lead to an increase in the availability of drivers based on incentivization. Quite simply, it encourages more drivers to get on the road, which in turn reduces the average person’s wait time back to nominal levels. To be sure, surge pricing approaches have been both lauded and reviled.
What is clear in this industry is that all pharmaceutical companies are for-profit entities, and therefore are invested in maximizing profit for their shareholders. Pharma as an industry has a significant R&D process and spend to fill pipelines with next-generation therapies, and many of these candidates will fail long before ever reaching the market. This financing of probabilities is extraordinarily expensive, and companies need to recoup their losses by establishing rational prices for the drugs that actually do succeed in gaining regulatory approval.
Dynamic pricing is one method of ensuring that companies stay competitive with the market and also can fund continuous innovation. The problem that develops, of course, is that manufacturers can rig the system to ‘short’ the supply to artificially increase demand rates to set dynamic surge pricing higher. There are various ways to address this eventuality in people gaming the system, but as Fermat opined, these solutions “won’t fit in these margins.” Suffice it to say that pricing approaches can’t remain the same as they are today, or the government and regulatory bodies will indeed step in and force the hand of a less-than-desirable future state.
But of course, another question that remains is how do we set the algorithm(s) for the dynamic pricing models? A good question. There are many ways to do so, some are best practices, and some are worst practices. Before a wholesale decree that dynamic pricing can’t work for healthcare treatments, such as drug therapies, because healthcare is ‘too altruistic’ of a product or service to conform to sterile economically-driven models of supply and demand, note that Uber itself shows how raising prices to incentivize drivers can lead to more reliable ride availability when, for example, people are leaving bars and restaurants late at night and are too drunk to drive. In certain cases, the ability for drivers to be paid more during off-hours means that more drivers will provide their services to the surge demand, and there will be fewer drunk drivers on the road, reducing accidents, injuries, and fatalities.4
Of course, there are many other ways to approach this issue for the industry, but it is an issue that we in fact need to collectively address before it becomes a “change that’s done to us.” There’s a wildly different perception in the world about the nature of a medicine that has been produced by a public company, and, for example, a smartphone. Both had R&D processes, incurred rigorous testing, marketing, and scrutiny of sales performance. But while society’s social contract allows the smart device to have an arbitrarily-assigned MSRP, medicine is thought of as different. Whether right or wrong, this is the challenge we’re faced with in the court of public opinion.
References
- The Economist. (2016). A fare shake. http://www.economist.com/news/finance-and-economics/21698656-jacking-up-prices-may-not-be-only-way-balance-supply-and-demand-taxis
- Uber. (2017). How surge pricing works. https://www.uber.com/info/how-surge-works/
- Surowiecki, J. (2014). In praise of efficient price gouging. MIT Technology Review. https://www.technologyreview.com/s/529961/in-praise-of-efficient-price-gouging/
- Liepman, L. (2016). DWI arrests spike after Uber/Lyft leave Austin. CBS Austin. http://cbsaustin.com/news/local/dwi-arrests-spike-after-uberlyft-leave-austin
Ben Locwin
Ben Locwin, PhD, MBA, is President of Healthcare Science Advisors. He is an expert media contact for the American Association of Pharmaceutical Scientists (AAPS) and is also on the Advisory Board for the Association for Talent Development’s (ATD) Healthcare Community of Practice, working on initiatives that are improving healthcare outcomes worldwide. Dr. Locwin has worked with several of the Top 10 pharma companies (both annual sales and market cap), and is currently creating improvements in the healthcare industry on patient-centricity. This is all critically important to the future of the industry, because we’re all (or will be) patients within the system. Improving the experience and ultimately, the outcomes, helps all of us. @BenLocwin.
